


Introduction
Ureteral duplication is a congenital anomaly in which the ureteric bud, the embryonic origin of the ureter, divides or occurs twice and connects two ureters to one kidney [1,2]. This is one of the most common urogenital malformations occurring in approximately 1% of the population; it can be accompanied by various clinical complications, such as vesicoureteral reflux (VUR), hydronephrosis, and ectopic ureter [1-3]. Previously, ureteral duplications were diagnosed during hospital visit for urinary tract infection or fever. More recently, in a Korean study published in 2003, 47% of patients with ureteral duplication were diagnosed with prenatal ultrasonography, and 36% were diagnosed during evaluation of fever or urinary tract infection, reflecting the changing process of ureteral duplication diagnosis [4].
The purpose of this study was to analyze the clinical characteristics of pediatric patients recently diagnosed with ureteral duplication and to compare the characteristics with those described in previous reports.
Material and methods
We retrospectively reviewed the medical records of 32 pediatric patients who were diagnosed with ureteral duplication at Kyungpook National University Hospital between January 2008 and June 2017. The initial diagnosis of ureteral duplication was usually made by ultrasonography, performed during the prenatal period in most cases. Intravenous pyelogram, the previous main diagnostic tool for ureteral duplication, was seldom performed due to the radiation risk and lack of additional benefit compared with ultrasonography. With ultrasonography, ureteral dilation, presence of ureterocele in the bladder, and severity of hydronephrosis were evaluated simultaneously. VUR was diagnosed only by voiding cystourethrogram. To distinguish between complete and incomplete types of ureteral duplication, additional evaluations including diuretic renogram and magnetic resonance urography were performed; diagnostic cystoscopy was performed to identify the orifice of the ectopic ureter in some patients. Additional data included the patientsŌĆÖ age, sex, clinical manifestations at initial diagnosis, type of duplex system, and other urological anomalies.
The StudentŌĆÖs t-test was used to analyze continuous variables. A P value <0.05 was considered statistically significant. All statistical analyses were performed with the R software, version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
During the study period, 32 infants and children were diagnosed with ureteral duplication at our hospital. Of them, 22 were female (68.7%) and 10 were male (31.3%). In 27 patients (84.4%), ureteral duplication was diagnosed before the age of 3 months and in 31 (96.9%), ureteral duplication was diagnosed during the first 12 months. In other words, most of these patients were first diagnosed with ureteral duplication by age three months, and almost all were diagnosed by age 12 months (Table 1).
Ureteral duplication was first detected by prenatal ultrasonography in 81.3% of the patients (n=26); in 15.6% (n=5), ureteral duplication was detected during a visit to the hospital due to fever and urinary tract infection. No patients presented with urinary incontinence due to ectopic ureter as an initial chief concern.
Because 4 of the 32 included patients (12.5%) were had bilateral ureteral duplication, a total of 36 occurrences of ureteral duplication were investigated. Among these, 17 occurrences (47.2%) were compatible with the complete type of ureteral duplication and 19 cases (52.8%) with the incomplete type. There was no significant difference between the right kidney to left kidney ratios: 9 to 8 for the complete type and 11 to 8 for the incomplete type (Table 1).
Other urinary tract anomalies associated with the complete type of ureteral duplication were: ureterocele in 7 cases (19.4% of total 36 cases/41% of 17 cases with the complete type), vesicoureteral reflux in 11 cases (30.6% of total 36 cases/65% of 17 cases with the complete type), and ectopic ureter in 5 cases (13.9% of total 36 cases/29% of 17 cases with the complete type). In contrast, among 19 cases of incomplete ureteral duplication, none was associated with ureterocele or VUR (Table 2).
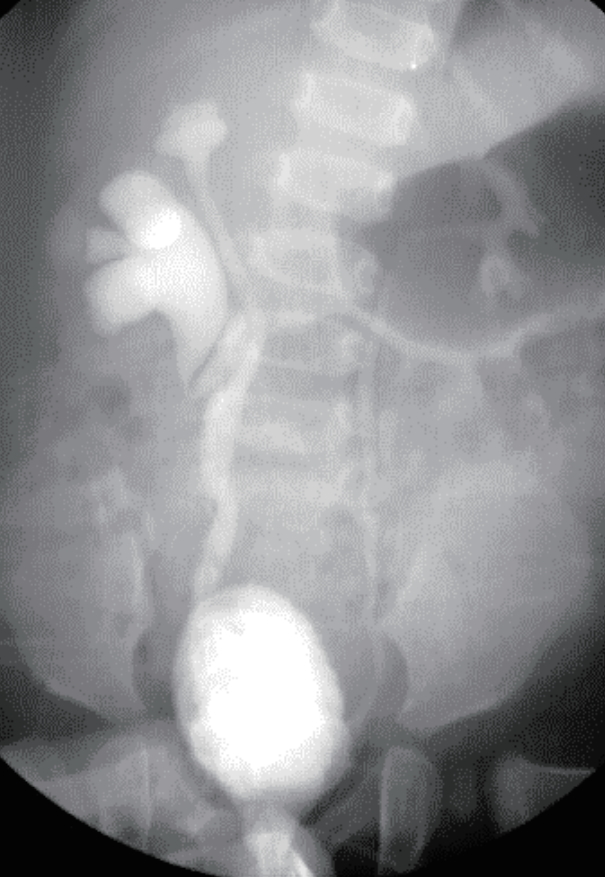
VUR was confirmed in the upper moiety of the ureteral duplication (2 cases), in the lower moiety (4 cases), in both the upper and lower moieties (2 cases), and in the upper and lower moieties of the ureteral duplication and the contralateral normal kidney (3 cases) (Table 3 and Fig. 1). Three cases of VUR were treated surgically (e.g., with ureteroneocystostomy), 4 cases were managed by observation and did not develop urinary tract infection or other complications, and in 4 cases, VUR resolved spontaneously.
In the 5 cases of ectopic ureter associated with ureteral duplication, the ectopic ureter was located in the bladder neck (2), urethra (2), and vagina (1) (Table 3). In all 7 cases with ureterocele, transurethral resection was performed, followed by ureteroureterostomy in 6 cases as the definitive operative treatment. Notably, one patient with ureterocele who underwent transurethral resection developed new VUR postoperatively.
Discussion
Ureteral duplication is the most common congenital anomaly of the urinary tract, with an estimated incidence in the general population of 0.8ŌĆō5% from autopsy studies [1,2,5]. The congenital malformation consists of two ureters connected to one kidney, resulting from duplication or division of the ureteric bud, the embryonic origin of the ureters [1,3]. The superior bud derives from the upper pole of a duplicated kidney and the inferior bud derives from the lower pole. Generally, superior bud is carried inferiorly along with any derivative of the distal mesonephric duct, so the ectopic ureter drains the upper pole of the duplicated kidney and the two ureters cross each other [6]. Therefore, the orifice of the ureter communicating with the upper pole in the complete type of ureteral duplication is located more medial and inferior than the normal position, but that of the ureter communicating with the lower pole is located more lateral and superior than the normal position, as described by the Weigert-Meyer rule [6-8]. As a result, dysplastic change and hydronephrosis due to ureteral obstruction more usually occur in the upper pole of a duplicated kidney, and VUR more usually occurs at the lower pole [6,9]. Incomplete type of ureteral duplication is thought to arise from premature bifurcation of the ureteric bud, before entering the metanephric blastema and not clinically significant in most cases [10].
In the past, ureteral duplication was diagnosed during hospital visits for urinary tract infection or fever, but more recently, the diagnosis was often made before the development of complication. In an article published in 2003 [4], 47% of cases of ureteral duplication were diagnosed by prenatal ultrasonography and 36 percent were diagnosed in patients with fever or urinary tract infection. In our study, 81.3% of cases were first detected by prenatal ultrasonography, and 15.6% were diagnosed during a visit to the hospital due to fever and urinary tract infection. Also, no patient visited the hospital with urinary incontinence due to an ectopic ureter as an initial chief concern. Our results show that ureteral duplication is being diagnosed earlier, by routine fetal ultrasound, than described in previous reports.
It has been reported that ureteral duplication generally occurs more commonly in female patients than in male patients, and this anomaly is bilateral in 17ŌĆō33% of cases. Additionally, a total of 60% of duplex systems have incomplete ureters duplication, with 40% showing complete ureteral duplication [1]. Similarly, in our study, female patients (68.7%) outnumbered male patients (31.3%), and incomplete types (52.8%) were more common than complete types (47.2%).
Most patients with incomplete types of ureteral duplication are clinically asymptomatic and the anomaly may be undetected. However, the complete type of ureteral duplication may be associated with an ectopic ureter, VUR, or ureterocele, and with symptoms such as obstruction, urinary incontinence, or urinary tract infection [11,12]. Accordingly, in our study, cases of complete ureteral duplication had accompanying by VUR, ureterocele, and ectopic ureter; in contrast, none of the incomplete type cases we evaluated had associated ureterocele or VUR.
VUR is more often found in association with ureteral duplication than in a single system and appears in 70% of patients with infection and ureteral duplication [13]. Low-grade VUR can be managed with antibiotics and careful observation, but high-grade VUR requires more intensive management. If kidney damage increases or antibiotic prevention fails, surgery must be performed [14]. In our study, 4 patients with high-grade VUR were treated surgically. 8 patients with low-grade VUR who were managed by observation, presented no urinary tract infection or spontaneous resolution of VUR.
Another malformation associated with ureteral duplication, ectopic ureter, occurs 2 to 3 times more commonly in female patients than in male patients [15]. When the urethra is located in the distal region of the sphincter, female patients may have urinary incontinence [15]. In this study, 5 cases of ectopic ureter were identified, of which 3 occurred in girls and 2 in boys.
Obstruction of the ureteral duplication most often occurs due to the presence of ureterocele [16]. This complication usually occurs 8 times more often in female patients than in male patients [17]. In our study, 7 cases of ureterocele were identified, including 6 cases in girls and 1 case in a boy. Initial and subsequent management of complete ureteral duplication with VUR or ureterocele has been controversial, and the management options have included partial nephrectomy, endoscopic decompression, and ureteroureterostomy [11,18,19]. The first-line procedure for ureterocele in neonatal patients is endoscopic puncture; accordingly, in all 7 cases of ureterocele in this study, a transurethral resection was performed and in 6 of these cases, ureteroureterostomy was performed as the definitive treatment for complete ureteral duplication.
In conclusion, this study shows that ureteral duplication is being detected earlier through the routine performance of prenatal ultrasonography and that conservative management is more common than surgical management. However, additional evaluation and treatment protocols are needed to overcome the limitations of ultrasonography, such as difficulties in identifying the type of duplication, presence of VUR, and location of the orifice of ectopic ureter.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




