


Introduction
Abnormal urinalysis (AUA) in children, characterized by any abnormal levels of certain substances, cells, or even microorganisms in the urine, is one of the most common reasons that patients are referred to nephrologists. AUA can range from asymptomatic to macroscopic hematuria; these can be caused by transient conditions, such as urinary tract infections (UTIs) or underlying chronic diseases, such as glomerulonephritis (GN) [1]. Since conditions that may cause AUA are diverse, their treatment and outcomes also vary. For example, the Alport syndrome does not respond to immunosuppressive management and invariably progresses to end-stage kidney disease, while lupus nephropathy requires prolonged immunosuppressants (IS), and postinfectious GN remits spontaneously. Moreover, benign conditions, such as nutcracker syndrome, which does not require management, may also present with AUA. Therefore, it is essential to obtain a precise diagnosis and manage the underlying condition that can be diagnosed through detailed history taking, including familial history, ultrasonography, blood and urine examination, and sometimes, kidney biopsy [2-5].
According to reports of school screening programs in East Asia, 0.01% to 5.10% of children had an AUA [6,7]. Isolated hematuria is the most common finding, comprising approximately two-thirds of the AUA cases [6,7]. Children with isolated hematuria are likely to have normal or benign etiology and good prognosis [8,9], whereas children with persistent combined hematuria and proteinuria are likely to have chronic GN [7,8,10]. When chronic GN is suspected, prompt management is required because it may progress to end-stage kidney disease, if left untreated. However, the management of GN often includes IS, which has significant side effects. Therefore, a definitive diagnosis is crucial before starting potentially harmful treatments, such as IS. This is reflected in international and national guidelines. The Kidney Disease: Improving Global Outcomes (KDIGO) guidelines in 2021 recommend that kidney biopsies be performed in patients with persistent glomerular hematuria and/or proteinuria [3]. A recently produced Korean guideline on hematuria in children also recommends kidney biopsies when persistent hematuria is accompanied by proteinuria, hypertension, or decreased kidney function [2]. However, not all pediatric nephrologists perform kidney biopsies before initiating IS. To assess the clinical practice pattern of AUA in children, we surveyed the opinions of members of the Korean Society of Pediatric Nephrology (KSPN) using a clinical vignette. Herein, we report the results of the survey along with a discussion.
Methods
A survey on clinical practice patterns using a clinical vignette was emailed to all KSPN members. The questionnaire is included in the supplementary documents of this study. Responses were analyzed using the proportions of each option. If respondents gave multiple answers to a question, they were considered as each answer.
Results
Characteristics of survey responders
A total of 32 clinicians (5.48% of the 584 recipients of the survey email) responded to the online survey; their characteristics are shown in Table 1. Of the 32 clinicians, 22 (68.8%) were certificated pediatric nephrologists, and 23 (71.9%) worked at a tertiary hospital. A quarter of the responders had less than 5 years of experience as pediatric nephrologists and another quarter had 11 to 20 years of experience (28.1%, 9/32). Three out of the 32 (9.38%) clinicians had >30 years of experience.
Responses to the survey
Clinical vignette part 1
A 12-year-old girl visited a hospital complaining of gross hematuria with proteinuria for 2 weeks. Her medical and family histories were unremarkable, except that she had gross hematuria and was treated with antibiotics for a suspected UTI 3 years ago. Urinalysis at school screening 3 months prior to admission was normal. Present illness of gross hematuria appeared 3 days after vaccination (influenza and Japanese encephalitis) with upper respiratory symptoms. The patient did not complain of dysuria or fever. Upon examination, the patient appeared physically well with height of a 155 cm (50ŌĆō75 percentile), weight of 40 kg (25ŌĆō50 percentile), and body mass index of 16.6 kg/m2. Her blood pressure was 117/80 mmHg (88/96 percentile). Urinalysis revealed proteinuria with hematuria of red blood cell (RBC) 50ŌĆō99/high-power field (HPF) with 13% dysmorphic RBCs but no pyuria. The urine protein-to-creatinine ratio (UPCR) was 1.32 mg/mg. Kidney function was normal, with urea nitrogen of 9.2 mg/dL and creatinine (Cr) of 0.45 mg/dL. Blood tests to rule out secondary causes were normal: complement component (C)3 was 105 mg/dL, C4 was 28 mg/dL, and the antinuclear antibody was negative. Kidney Doppler ultrasonography revealed normal cortical echogenicity and flow. The most common answer to the question of probable diagnosis was immunoglobulin A nephropathy (IgAN; 87.5%, 28/32), followed by postinfectious GN, Alport syndrome, thin glomerular basement membrane disease, and lupus nephritis. UTIs, such as cystitis, were also suspected.
Clinical vignette part 2
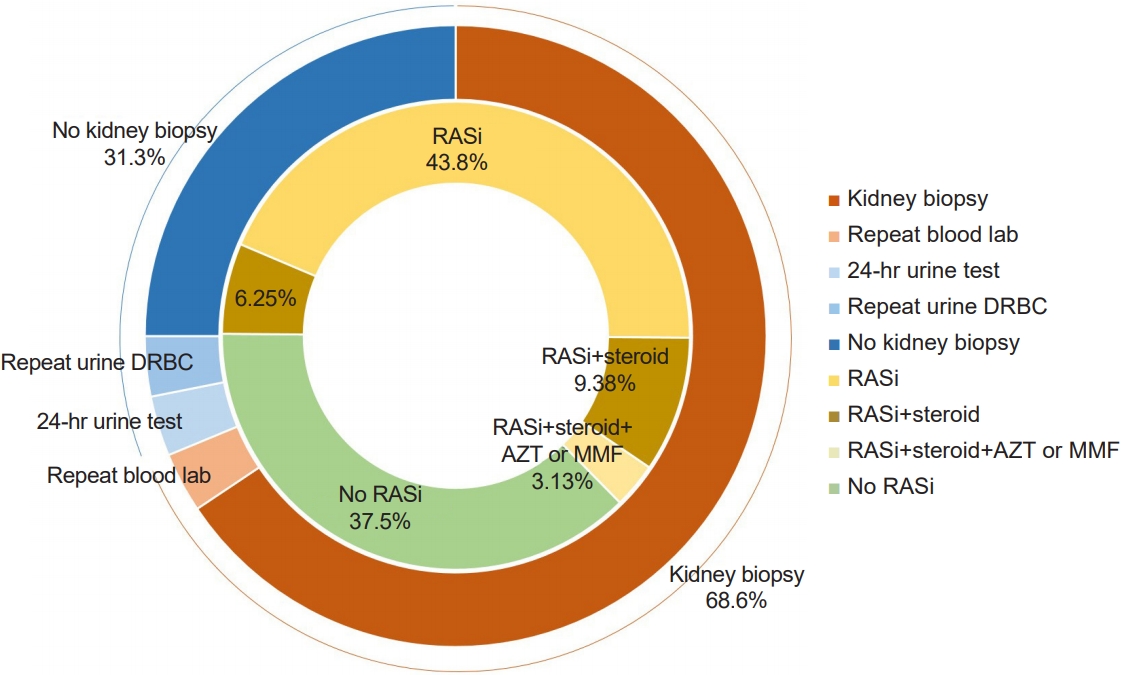
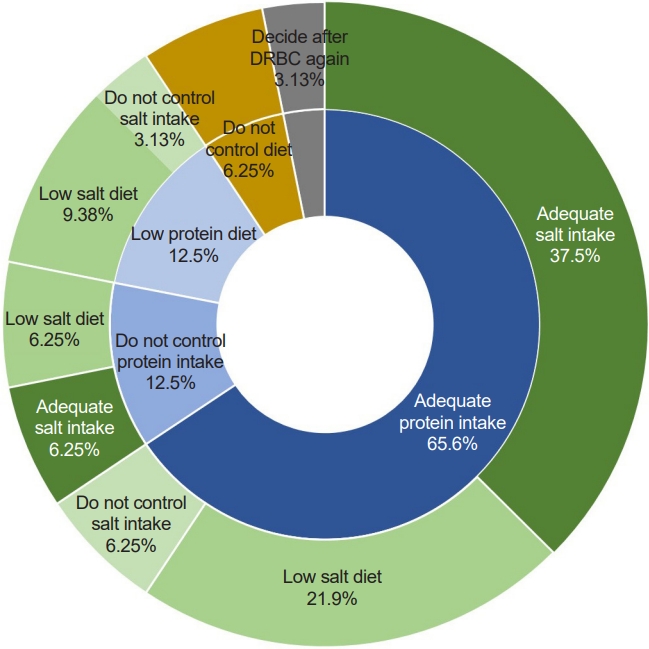
Two weeks later, she still had proteinuria (UPCR 1.52 mg/mg) and hematuria (urine RBC 20ŌĆō49/HPF) with estimated glomerular filtration ratio (eGFR) 103 mL/min/1.73 m2 (Cr 0.45 mg/dL and cystatin C [CysC] 0.93 mg/dL). When asked what to do next for persistent hematuria and proteinuria, approximately two-thirds of the responders answered a kidney biopsy (68.8%, 22/32) and renin-angiotensin system (RAS) inhibition by angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (62.5%, 20/32) (Fig. 1). Six responders (18.8%) replied that they would use steroids with (n=4, 12.5%) or without kidney biopsy (n=2, 6.25%). Regarding the question about a dietary recommendation, responders mostly answered that they would recommend protein intake as much as dietary reference intakes (DRIs; 65.6%, 21/32), and 12 (37.5%) of them also recommend sodium intake as DRIs. In contrast, 12 (37.5%) answered that they recommended a low-salt diet. Two physicians answered that no dietary control was required (Fig. 2).
Clinical vignette part 3
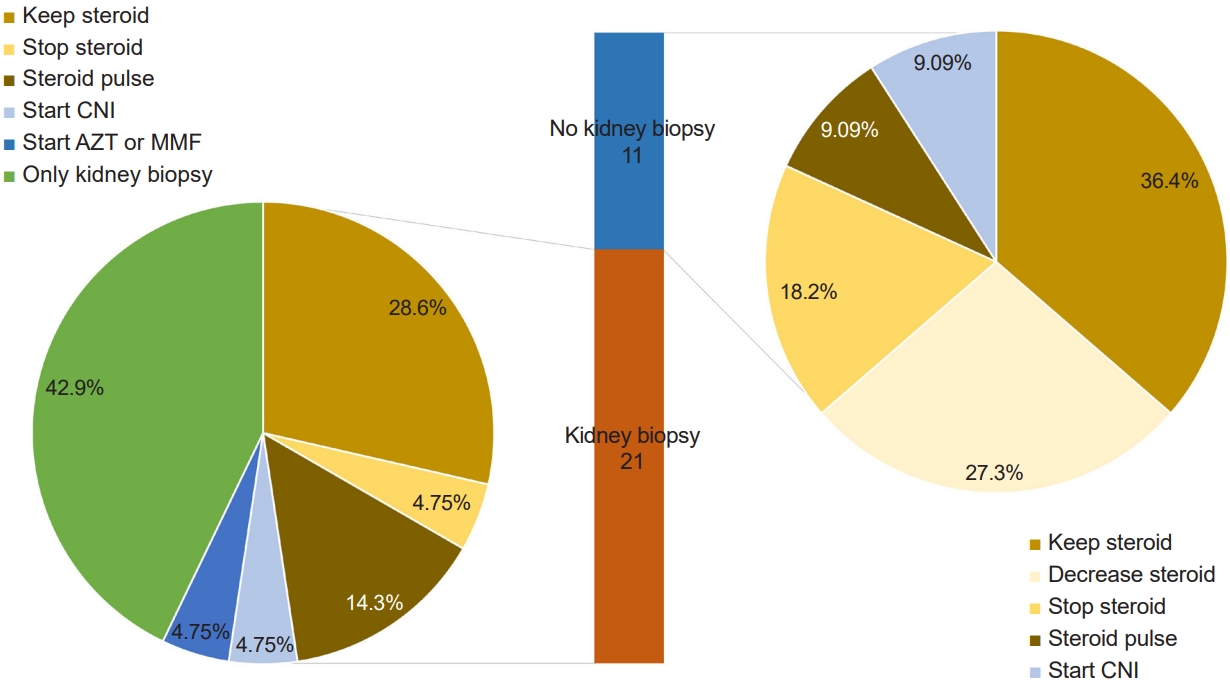
She was prescribed prednisolone 30 mg/day and enalapril 5 mg/day. After 2 weeks, proteinuria (UPCR 1.48 mg/mg) and hematuria (urine RBC 5ŌĆō9/HPF) persisted. Kidney function improved with Cr 0.45 mg/dL and eGFR 142 mL/min/1.73 m2. Regarding the question of what to do next, 21 responders (65.6%) answered kidney biopsies, 18 of whom were nephrologists. Approximately one-third (37.5%, 12/32) answered that they would retain steroids, and three (9.38%) said that they would decrease or stop steroids. Four (12.5%) responded that they would administer steroid pulses, of whom only one was a nephrologist. Two (6.25%) answered that they would start calcineurin inhibitors, and one would start azathioprine or mycophenolate mofetil (MMF) (Fig. 3).
Clinical vignette part 4
She was managed with the same medication for another 3 weeks, but proteinuria (UPCR 1.01 mg/mg) and hematuria (urine RBC 11ŌĆō20/HPF) did not disappear. She was then administered methylprednisolone pulses (500 mg per day for 3 consecutive days) and cyclosporine. Following the pulse, the patient continued taking deflazacort 12 tablets (72 mg) once a day, cyclosporine 75 mg twice a day, and enalapril (7.5 mg) once a day. Hematuria and proteinuria persisted, and kidney function was preserved. She was instructed to restrict dietary protein and salt intake. Six weeks later, her UPCR was 0.24 mg/mg and her urine RBC was 1ŌĆō4/HPF with Cr 0.48 mg/dL and CysC 0.89 mg/dL (eGFR 101 mL/min/1.73 m2). The patient had a cushingoid and hairy appearance. In response to these findings, 27 responders (84.4%) said they would decrease the steroid levels, half of whom stopped cyclosporine. Eight (25.0%) responded to perform kidney biopsy with steroid decrease, and one to administer azathioprine or MMF.
Clinical vignette part 5
Six weeks after initiating steroid therapy, the patient visited another hospital for a second opinion. At the second hospital, proteinuria was minimal (UPCR 0.22 mg/mg), and there was no hematuria (urine RBC 1ŌĆō4/HPF). The cyclosporine and steroids were discontinued. One week later, proteinuria disappeared (UPCR 0.13 mg/mg), and hematuria did not recur. Kidney function also improved with Cr 0.5 mg/dL, CysC 0.65 mg/dL, and eGFR 124 mL/min/1.73 m2. When asked about respondersŌĆÖ opinions about clinical practices, one-third of responders (36.4%, 4/11) emphasized the necessity of kidney biopsies to diagnose the underlying disease and decide the treatment regimen. Another four answered that RAS blockage should be maintained, and proteinuria and hematuria should be observed. One recommended that explanation should be provided for the adverse effects of IS treatment on children before initiating it.
Discussion
This survey revealed that the clinical practice patterns of AUA in children are diverse. Although about 5% of the email recipients responded to the survey, we assume that the survey captured the opinions of more than half of the active members of the KSPN, considering that the total number of active, certified pediatric nephrologists in Korea is approximately 40, and the responderŌĆÖs experience and age are not concentrated. When comparing the responses of nephrologists and others, the most prominent difference was that most nephrologists chose to perform a kidney biopsy before starting any treatment, whereas the others were willing to perform a steroid pulse even without a kidney biopsy.
The initial part of the survey assessed practice patterns of the diagnostic approach. While most responders suspected GN, only two-thirds answered that they had performed kidney biopsies. However, kidney biopsy is essential for the diagnosis of GN since the clinical presentation itself is not different between various glomerulopathies, including genetic diseases. Kidney biopsy is an invasive procedure that may lead to complications, such as hematuria, hematoma, arteriovenous fistula, and even loss of the kidney [11,12]. In addition, approximately 15% of the children who undergo kidney biopsies may not obtain positive results [13,14]. Those were why clinicians are reluctant to kidney biopsies. Of course, it is possible to diagnose GN through biomarkers (phospholipase A2 receptor antibody in membranous nephropathy or myeloperoxidase in antineutrophil cytoplasmic antibody vasculitis) and genetic tests in the Alport disease or Fabry disease or by diagnosing systemic diseases, such as systemic lupus erythematosus [3]. However, the clinical vignette of the survey was not compatible with any situation in which a biopsy could be exempted. Suspected cases of GN require a kidney biopsy as an accurate diagnosis could change treatment and prognosis [15].
The treatment for hematuria is based on the underlying disease, not the hematuria itself. RAS inhibition is recommended as the first-line treatment when a child was diagnosed with GN, such as IgAN [3], as our responders chose. In the same situation, six responders answered to start steroids. However, because IS are accompanied by immune suppression and complications, such as growth suppression, cushingoid features, and osteoporosis [16], IS should only be used when indicated even after a definitive diagnosis. According to the KDIGO and Japanese guidelines for IgAN, even if a patient is diagnosed with IgAN, IS are recommended when patients are at a high risk of chronic kidney disease (CKD): severe proteinuria despite RAS blockage or mesangial hypercellularity in a kidney biopsy [3,17].
Similarly, steroid pulse therapy is considered when patients are indicated. The clinical vignette of the survey was managed with steroid pulse therapy when proteinuria persisted despite 5 weeks of oral steroids, and four responders agreed with this. However, methylprednisolone pulse therapy as early treatment is indicated only for steroid-resistant nephrotic syndrome and lupus nephritis. In IgAN, one study assessed the efficacy of steroid pulse therapy. Pozzi et al. [18] reported that intravenous high-dose methylprednisolone (1 g/day for 3 consecutive days, every 2 months) followed by oral prednisolone for 6 months was effective in decreasing proteinuria, but the indication of steroid pulse therapy in this study persisted for more than 1 g/day for more than 3 months. In contrast to pediatric nephrotic syndrome, remission of proteinuria occurs far later than weeks in the majority of GN cases, as reflected by KDIGO recommending first-line treatment for 6 months for most types of GN [3]. Likewise, the endpoints of clinical trials on IgAN are remission rates at 6 months after treatment, including the global study on the effectiveness of oral methylprednisolone in IgAN [19] and two clinical trials comparing steroid plus ACEi with ACEi alone in proteinuria in IgAN [20,21]. Therefore, even when we had the pathologic diagnosis of GN, aggressive IS are indicated only when the disease is active despite treatment with less toxic management for months not weeks [3]. If we consider nonsteroidal IS treatment, such as with cyclosporine or MMF, we need a clear indication, such as a pathologic diagnosis of IgAN with diffuse mesangial proliferation, as recommended by the Japanese guidelines, because these medications may accompany serious complications [17].
When managing children with AUA or kidney disease, one of the most common questions which patients ask to physicians is how to modify their diet. Often, the parents of children with supposedly kidney disease restrict salt and protein intake from the diet of the children, following the general recommendation of adult patients with CKD. However, there is no evidence supporting dietary restriction in children with AUA or GN if the patient does not have hypertension or edema [4]. Salt restriction may be helpful in patients with hematuria due to hypercalciuria [22]. In addition, as high salt intake is associated with high blood pressure [23,24], in children with CKD, salt restriction is recommended to the extent that it does not hinder growth in cases of hypertension [25]. Otherwise, restricting salt intake does not help children with AUA. In contrast, restricting protein is not recommended even in children with CKD because there is no evidence that protein restriction can delay disease progression but only undermine growth [26]. Therefore, Uauy et al. [27] recommended that children consume as much protein as DRIs for their age. The most important consideration when recommending dietary modification for pediatric patients is that growth should not be hindered.
There were several limitations to this study. To the best of our knowledge, this is the first survey in Korea on clinical practice patterns for children with AUA. However, although most active members of the KSPN participated in the survey, the number of survey responders was too small, and not all members were included. In addition, the survey was conducted based on the clinical vignette, which may not have accurately reflected actual clinical practice in all situations. Therefore, future research should aim to survey a larger, more representative sample, and use more comprehensive survey instruments to obtain clearer results.
Although the number of survey responders was small, the survey provided valuable insight into the clinical approach of healthcare providers when managing children with AUA. Clinicians typically suspected IgAN when children showed hematuria and proteinuria, and were willing to perform a kidney biopsy. The most common treatment chosen was RAS inhibition, with or without steroids. Regarding protein intake, most responders recommended consuming DRIs. However, for salt intake, half of the responders recommended following a low-salt diet, while the other half recommended consuming as DRIs.
ChildrenŌĆÖs AUA is a common condition that has various causes, treatments, and prognoses. Since the treatment of AUA depends on the underlying etiology, such as GN, a definite diagnostic approach is needed, including a kidney biopsy. IS, which is usually included in the treatment of GN, have many adverse effects. Therefore, before using IS, it is necessary to confirm an accurate diagnosis and indications. Lastly, when recommending a diet to children with AUA or suspected GN, although evidence is insufficient, the priority should be to ensure that growth is not interrupted.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




